
Why Is Your Implant So Expensive?
A Field Guide for the Question You'll Always Face


Years ago I carried a system for odontoid fracture fixation called the Apfelbaum Odontoid System. Most odontoid fractures can be treated without surgery, but for those patients who did need an operation, the Apfelbaum was the only FDA-indicated system on the market — the unambiguous go-to for these procedures.
It wasn’t a case I covered often, and when I did, it was a pain. My surgeons and I would review the steps each time as though we were doing it for the first time — because, effectively, we were. Since it wasn’t a system we kept on the shelf, it had to be ordered in, usually at the last minute.
One particular afternoon, my surgeon called with the kind of excitement that is contagious right up until you hear the details: he had just added a Type III odontoid fracture case for 7:30 the next morning. To make it happen, our operations team quickly packaged a set and dispatched it via FedEx’s most expensive next-flight-out shipping — white glove, courier-handled, no-expense-spared. For those unfamiliar, booking NFO shipping is the logistical equivalent of buying a last-minute cross-country plane ticket.
I showed up the next morning to a hospital two hours from my house, running on too little sleep after a night of calls with the courier, dispatcher, and the hospital.
Then the case cancelled.
And that’s when my surgeon — the same man I had just moved heaven and earth for — looked up and said: “Sorry we didn’t get to do this one. By the way, why does this screw cost $3,000? It’s just a lag screw, for crying out loud.”
I can’t remember exactly how I responded. What I can tell you is that I likely failed to fully contain my irritation, and I failed just as thoroughly to explain why that implant cost what it cost. I mentioned the NFO shipping we’d have to absorb, the hoops I’d jumped through, and the fact that our company would lose money on this case (and most odontoid cases for that matter). All true. All beside the point.
Looking back, I could have done so much better.
There’s a question that will find you. It doesn’t matter whether you’re standing in a scrub sink conversation, sitting across a Value Analysis Committee table, or getting a side-eye from a purchasing manager holding your latest price sheet. It will come. And when it does, how you answer will say more about your credibility than anything else you do that day.
“Why is this implant so expensive?”
Most reps treat this question like a hazard to navigate — a pothole to swerve around, a personal accusation to deflect. That’s a mistake. The best salespeople treat it as something rarer and more valuable: an invitation to educate.
When we feel put on the spot, we default to one of two dysfunctional patterns. We either go defensive (”I don’t set the price — that’s above my pay grade”) or we go dismissive (”It’s worth it, trust me”). Both responses signal to your customer that you either don’t know the answer, or you don’t care enough to explain it. Neither builds trust. Both kill relationships.
The opportunity hiding inside this objection is enormous. And almost no one takes it.
The 2% Problem
Before we talk about what to say, let’s talk about what’s actually true. You can’t educate someone with a story you don’t believe yourself.
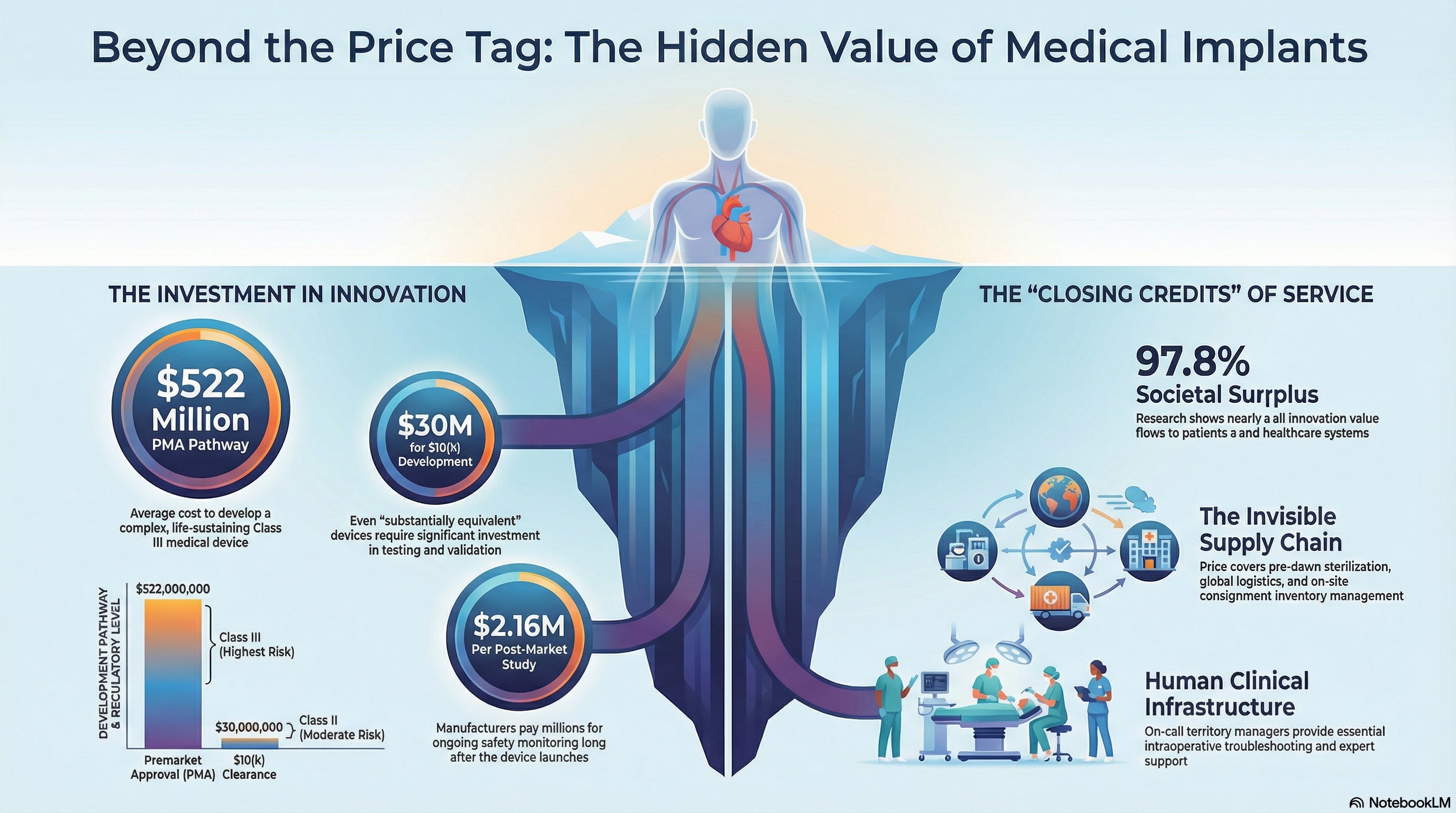
Nobel Prize-winning economist William Nordhaus spent years studying the economics of technological innovation. His conclusion was startling: the creators of technology capture only about 2.2% of the total social surplus from innovation. The other 97.8% flows to society — to patients who get their mobility back, to surgeons who operate with greater precision, to healthcare systems that spend less managing complications.
Think about that for a moment. The company that spent years developing the implant your surgeon just used — they’re keeping less than 3 cents of every dollar of value created. You’re not in a room full of people being gouged. You’re in a room where most people have no idea how much invisible work, risk, and capital went into putting that tray on the back table.
That’s your job. You’re the only one who can tell this story.
What It Actually Costs to Build What You Sell
Here’s where most reps fail: they’ve never thought through the full economics of what they’re selling. They know the feature set. They know the clinical data. But they couldn’t tell you — with any confidence — what it costs to bring a device to market.
So let’s walk through it.
The R&D Bill — And Why Not All Devices Are Created Equal
The FDA uses a tiered classification system, and the cost structure changes dramatically depending on where a device lands.
The most complex pathway is the Premarket Approval (PMA) — required for Class III devices like implantable cardiac pacemakers or novel joint replacement systems. These are the devices that sustain or support life and carry the highest patient risk. When accounting for failed programs and cost of capital, the mean capitalized development cost for a therapeutic complex Class III device is $522 million. That figure includes all the dead ends — the prototypes that didn’t survive bench testing, the trials that didn’t reach statistical significance, the innovations that never reached patients at all.
But a large portion of medical devices — including many products sold by reps reading this article — reach the market through a different pathway: the 510(k) clearance process. The 510(k) route is available when a device is substantially equivalent to a previously cleared predicate. Because you’re building on an established foundation rather than starting from scratch, the development costs are meaningfully lower. Bringing a Class II 510(k)-cleared device to market typically requires around $30 million in total company funding, with $2–5 million on development and engineering.
That’s a big difference. And it matters to your story.
If your product went through 510(k), be honest about that. You don’t need to pretend every implant you sell cost half a billion dollars to develop. What you should be able to explain is why the 510(k) framework still represents real investment: building on a predicate device isn’t free, and the testing, regulatory work, manufacturing validation, and quality systems required to reach clearance are still substantial. The price reflects that work — plus everything that comes after approval.
The Regulatory Gauntlet (It Doesn’t End at Clearance)
Whether your device came through PMA or 510(k), FDA oversight doesn’t stop at approval. Post-market surveillance is ongoing and expensive. FDA-mandated post-approval studies have shown a median cost of $2.16 million per study, and manufacturers may run multiple studies across their portfolio simultaneously. That ongoing investment in monitoring device safety and performance for years — sometimes decades — after launch is real money, and it’s baked into the price of the device.
The Hidden Costs That Never Make the Brochure
There’s a category of costs so embedded in daily operations that nobody highlights them externally. These are the costs of keeping the system running.
Think about the logistics ecosystem behind a single surgical case: trays of instruments delivered to the hospital before dawn to be sterilized, a distribution network that can reroute a shipment when a backorder materializes the night before an OR schedule, field inventory sitting on consignment in hospital storage rooms across dozens of accounts. When hospitals experiment with going “rep-less,” they discover quickly that they have to hire additional staff to pick up the slack — because the rep-supported model was never just a sales model. It was a service model with real operational value.
Add the clinical support infrastructure. Territory managers, clinical specialists, and regional account teams exist to make every case go smoothly, to troubleshoot intraoperatively, and to be the person the surgeon calls at 6am when the schedule shifts. That team is part of what your customer is buying — even when they don’t realize it.
When you add it all up — R&D, clinical evidence, regulatory clearance, post-market oversight, manufacturing, quality systems, logistics, field support, and the cost of the programs that didn’t make it — the price of the implant in that OR tray starts to tell a very different story.
How Not to Answer (A Hall of Shame)
Let’s be honest about why reps give bad answers to this question. It’s not usually because they don’t care. It’s because they’re uncomfortable, underprepared, or have miscalibrated their confidence-to-knowledge ratio. Here are some greatest hits from the field — each one a real thing a real rep has said, and each one a small masterpiece of what not to do.
“Doc, what do you say when a patient asks why the procedure is so expensive?” Bold strategy: when someone asks you a hard question, immediately ask them a harder question. You’ve successfully redirected the discomfort and learned nothing. The surgeon now knows you didn’t bring an answer — and they will remember.
“I notice you have the latest iPhone. Did you ask the Apple Store rep why it was so expensive?” Ah yes, the “actually, have you considered that you’re a hypocrite?” gambit. Technically provocative. Practically catastrophic. The surgeon spent eight years in medical school and another five in residency. They can handle a nuanced economic argument. They cannot handle being compared unfavorably to a consumer at the Genius Bar.
“We’re the only company with this technology on the market, so that’s why.” Accurate. Technically not wrong. Also the conversational equivalent of answering “What time is it?” with “Time exists.” You’ve stated a fact and explained nothing. Congratulations on your monopoly. Now justify it.
“I don’t set the price, Doc. Those decisions are way above my pay grade. I just work here.” This one is the rep equivalent of a shrug emoji. You’ve just told your customer that you are a human order form with a company car. If pricing decisions are above your pay grade, what exactly is within it? This is the moment the surgeon starts wondering whether they really need you in the room.
“If price is all you’re thinking about, I guess patient outcomes aren’t your priority.” No. Just no. The sentence that most reliably turns a price objection into a permanent relationship ending. Filed under: Things That Felt Clever in Your Head and Landed Like a Wrecking Ball in the Room.
Here’s the through-line in all five responses: they treat the question as an irritant rather than an opportunity. Research on expertise and persuasion consistently shows that people trust advisors who explain their reasoning. When you can explain why something costs what it costs, you signal mastery. When you deflect, you signal the opposite.
You Are the Closing Credits
Here’s a metaphor that tends to land.
The films you love all close with a wall of credits that runs for minutes — hundreds of names representing hundreds of people whose work you relied on entirely and will never think about again. The gaffer. The sound editor. The visual effects coordinator. The catering company that kept the cast functional during a six-week shoot.
Medical devices have no closing credits. Nobody sees the regulatory affairs team that spent two years shepherding the 510(k). Nobody meets the biomedical engineers who ran failure analysis on dozens of prototypes. Nobody thanks the quality systems manager who signs off on every production batch. The surgeon picks up the instrument knowing it will work. They just don’t know why it works — or what it cost to make it reliable.
That’s your job. You are the closing credits. You are the human through whom all of that invisible work becomes visible.
The most effective reps don’t just sell a product. They narrate the journey it took to get there. And when they do, the price tag doesn’t look like a number someone typed into a spreadsheet. It looks like what it actually is: the compressed sum of years of effort, expertise, and risk.
Know Your Core Message — Then Repeat It
The evidence on organizational communication is clear: the most effective messages are simple and repeated relentlessly.
When Kevin Lobo became CEO of Stryker, his team developed an eleven-word mission statement — “Together with our customers, we are driven to make healthcare better” — and he used it at the start of every presentation he gave. The combination of simplicity and repetition helped it spread organically, until presentations within Stryker routinely started with the mission. He once noted that he can travel anywhere in the world, ask employees to recite the mission, and 90% of the time they’ll get every word right — because it’s only eleven words.
The lesson: you need a message, not a monologue. When someone asks why your technology costs what it costs, you shouldn’t deliver a fifteen-minute lecture on FDA pathways. You should have a concise, repeatable story — three or four sentences — that anchors the conversation in reality and invites deeper discussion.
Something like:
“That’s a fair question. Most people don’t realize what goes into getting a device like this to market — the development, the regulatory process, the ongoing surveillance after clearance. There’s also a significant service infrastructure behind every case: logistics, field support, quality systems that run continuously. What you’re buying isn’t just the implant. It’s everything that had to happen to make it trustworthy, and everything that keeps it that way.”
Then stop. Let them respond. The best educators ask as many questions as they answer.
And then, critically: say it again next time. And the time after that. Repetition doesn’t make you sound like a broken record. It makes you sound like an expert. Over time, your customers will start repeating your ideas back to you — which is the surest sign that education has occurred.
The Long Game
Here’s the deeper insight that most sales training misses.
When you answer “Why is this so expensive?” with honesty and calm — without defensiveness, without deflection, without condescension — you’re not just handling an objection. You’re demonstrating something about your character that customers remember long after they’ve forgotten the conversation.
You’re showing them you understand the full picture of what you’re selling. You’re showing them you respect their intelligence enough to give a real answer. You’re showing them that you see yourself as a partner in their work, not a transaction to complete.
Trust in professional relationships is built not through agreement but through consistent, honest engagement. The reps who build durable relationships with surgeons and hospital systems aren’t the ones who never get asked hard questions. They’re the ones who welcome hard questions because they’ve done the work to answer them.
The question “Why is this so expensive?” is not your adversary. It’s your invitation.
Accept it.
Quick Reference: The Economics of What You Sell
The R&D Spectrum Class III PMA devices can cost $500M+ to bring to market when accounting for failed programs and cost of capital. Class II 510(k) devices are significantly less — typically $2–30M in development — but still represent real investment in testing, validation, and regulatory work.
The 510(k) Nuance “Substantially equivalent” doesn’t mean “free.” It means building on established science rather than reinventing it — which is efficient, not cheap.
Post-Market Surveillance FDA-mandated studies after clearance cost manufacturers an average of $2M per study. This monitoring runs for the commercial life of the device.
The Supply Chain Pre-dawn deliveries. Consignment inventory. Last-minute rerouting. These are services the device price supports, even when they’re invisible.
Field Support Territory managers, clinical specialists, and account teams make every case run smoothly. That team is part of the value proposition — whether or not the customer realizes it.
The Cost of Failure For every device that reached the OR, others didn’t make it. The cost of innovation includes the cost of the programs that failed. Successful products carry that burden.
The next time someone asks why your implant is so expensive, remember: you’re not defending a price. You’re honoring the work of every person whose contribution never made the credits.
That’s a story worth telling. Make sure you know it cold. Repeat as necessary.