
Is Your Surgeon Overpaid?
No. And here's a study your surgeon will actually read — and then buy you a coffee for sharing.

Every few years, a journalist somewhere discovers that American doctors (including your surgeons) make more money than doctors in other countries, and the think-pieces start flying.
The argument goes something like this: US healthcare costs nearly 18% of GDP — more than any other developed nation by a wide margin. Doctors are among the highest-paid professionals in the country. Therefore, doctors are a big part of why healthcare is so expensive. Therefore, if we just paid doctors less, healthcare would become more affordable.
It’s clean. It’s intuitive. It’s mostly wrong.
And as someone who sells medical technology into the clinical environments where these physicians work — who has watched a spine surgeon spend four hours on their feet reconstructing a shattered vertebra at 6am on a Saturday — you may have a strong gut reaction to that argument. You should. But gut reactions don’t win policy debates, and they don’t impress the physicians who ask you about this stuff. Data does.
So let’s look at the data.
A Brand-New Study Just Dropped. Here’s What It Actually Says.
In March 2026, researchers from the University of Chicago, Stanford, the University of Toronto, and several other institutions published a working paper through the National Bureau of Economic Research comparing physician incomes across four countries: the United States, Canada, the Netherlands, and Sweden. They used actual administrative tax data — not surveys, not estimates — covering hundreds of thousands of physicians in each country.
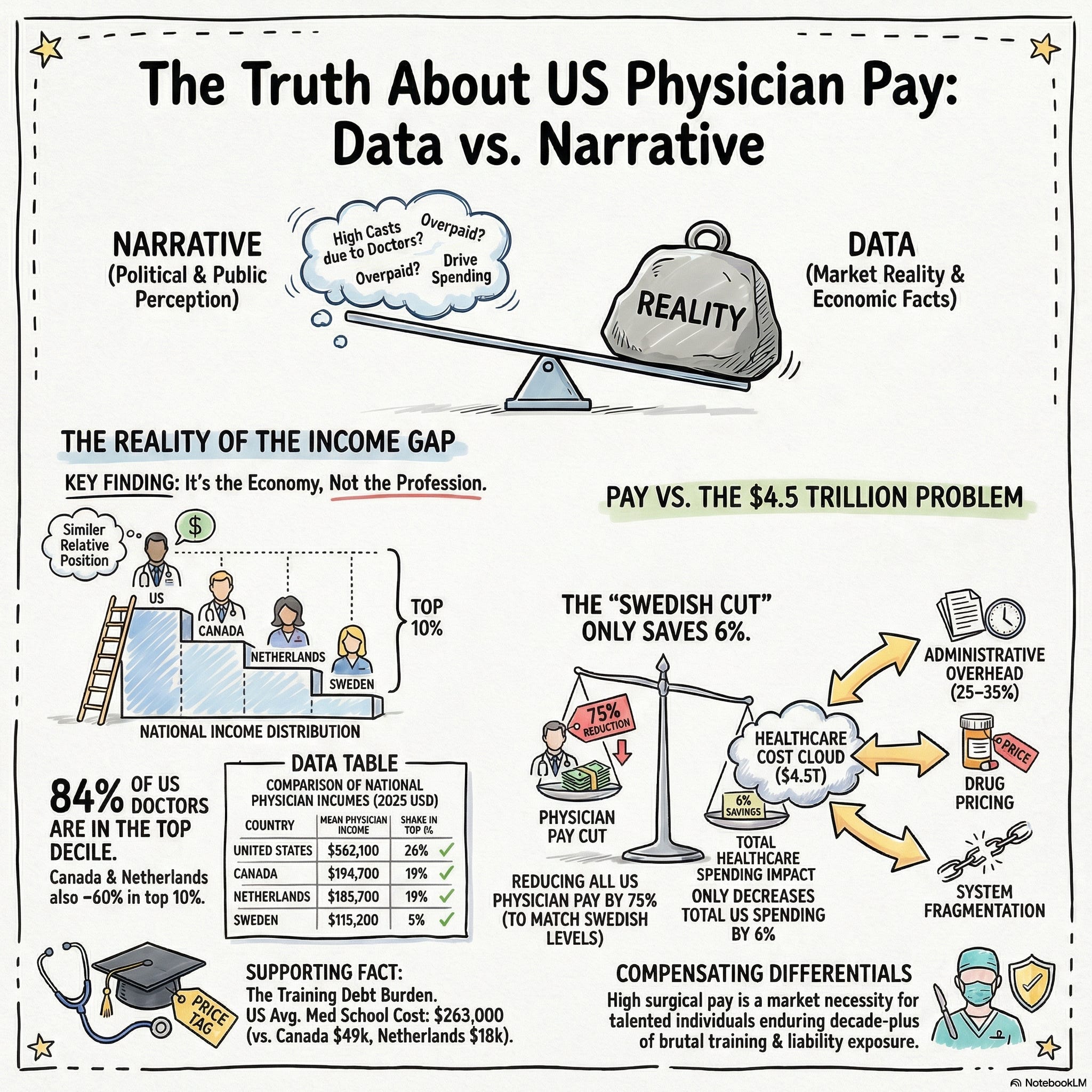
The headline numbers are striking. Average US physician income comes in at $562,100 — more than twice the Canadian figure of $194,700, three times the Netherlands at $185,700, and nearly five times Sweden at $115,200. On its face, that looks like Exhibit A for the “American doctors are overpaid” argument.
But here’s where it gets interesting.
The researchers didn’t just compare raw income figures. They looked at where physicians sit within their own country’s income distribution. And what they found reframes the entire conversation.
In all four countries, physicians are clustered at the top of the national income ladder. In the US, 84% of physicians are in the top decile of earners. In Canada and the Netherlands, it’s about 62%. In Sweden, about 60%. These are high-earning professionals everywhere — not just in America.
The real difference isn’t that American physicians occupy a dramatically higher relative position in their income distribution. It’s that the American income distribution itself is far more stretched at the top. The incomes at the 95th, 98th, and 99th percentiles of the US population are simply much higher than the corresponding percentiles in Canada, Sweden, or the Netherlands.
When the researchers ran the numbers — asking what would happen to average US physician income if you kept American income levels but redistributed physicians to match the relative positions of, say, Canadian doctors — it explained at most 22% of the gap. The rest? That’s not about how physicians are valued relative to their peers. That’s about how the entire US economy is structured.
In plain English: US doctors aren’t paid more because someone decided to overpay them. They’re paid more because everyone at the top of the American economy earns more. Surgeons compete in the same labor market as tech executives, finance professionals, and law partners. Their compensation reflects that market.
The Specialty Gap Is Real — And Makes Complete Sense
The study also breaks down physician income by specialty, and the patterns are consistent across all four countries. Specialists out-earn primary care physicians everywhere. Surgeons sit at or near the very top everywhere.
In the US, 42% of all specialists sit in the top 1% of national earners. In Canada it’s 27%. In the Netherlands, 21%. In Sweden, 7% — which reflects that country’s predominantly salaried, public-sector healthcare model.
None of this should surprise anyone who has spent time in an operating room. The training pipeline for a neurosurgeon, a spine surgeon, or a cardiac surgeon is brutal by any reasonable standard. Four years of college. Four years of medical school — at an average cost of $263,000 in the US, compared to $49,000 in Canada or $18,000 in the Netherlands. Residency ranging from four to seven years. Often a fellowship on top of that. A decade or more of post-graduate training before they do their first case independently. And once they’re in practice, the hours, the on-call demands, the liability exposure, and the emotional weight of the work don’t let up.
The income premium for surgical specialists isn’t an accident or an anomaly. It’s a compensating differential — the market’s way of ensuring that enough talented people are willing to go through what it takes to become one.
But Wait — If Doctors Aren’t the Problem, What Is?
Here’s where the honest conversation gets more uncomfortable — because the answer is “a lot of things, none of them simple.”
US healthcare spending is closing in on 20% of GDP. That’s somewhere north of $4.5 trillion a year. The researchers in this study ran a provocative counterfactual: what if you cut every US physician’s income to match the Swedish average? How much would you save?
The answer: about 6% of total healthcare spending. $291 billion sounds like a lot until you realize it would require reducing average physician income by 75% — a $342,900 pay cut per doctor. The researchers note, carefully, that this would likely reshape who chooses to enter medicine entirely. You’d save money on the back end while potentially hollowing out the pipeline on the front end.
Shift US physicians to merely match the relative income distribution of Swedish doctors — not the absolute levels, just the distribution — and you’re looking at a 3.8% reduction in total spending. $195 billion, with a 50% cut in average physician income.
These are not small numbers. But they are also not the answer to a system that costs $4.5 trillion a year.
So where is the waste? Researchers, policy analysts, and healthcare economists who study this seriously tend to point at several consistent targets: administrative overhead, which eats an estimated 25–35% of every healthcare dollar and runs far higher in the US than in any comparable system; drug pricing, which is structurally different in the US than everywhere else because the government does not negotiate prices; end-of-life care, which accounts for a disproportionate share of total spending; and fragmentation — a system built from hundreds of disconnected payers, providers, and systems rather than a coherent whole.
Physician compensation is a line item in a very large, very complicated budget. It is not the line item that explains why we spend twice what Canada spends per person.
What This Means for You
You already know that healthcare cost conversations don’t stay in policy journals. They show up in Value Analysis Committee meetings. They show up in hospital budget cycles. They show up when a purchasing manager slides your price sheet across the table and raises an eyebrow. And occasionally — more often than you might expect — they show up when a surgeon, in a quiet moment between cases, says something like: “They keep talking about cutting physician reimbursement. I’m getting a little tired of being the villain in this story.”
That moment is an opening.
Not to launch into a policy lecture. Not to hand them a printout. But to be the person in their professional orbit who actually understands the economics of their world — and who can say, with confidence: “There’s actually a really interesting study on this…”
That’s the kind of conversation that doesn’t get forgotten. It doesn’t show up on a call report. It doesn’t close a deal that afternoon. But it builds the kind of trust that makes you the rep they call first, recommend loudest, and fight to keep in their OR when someone in administration tries to go rep-less.
The Bottom Line
US physicians — your customers, your surgeon partners, the people who rely on your product knowledge at 6am in a room where the stakes don’t get any higher — are not the reason American healthcare is expensive. They are highly compensated professionals in a highly compensated economy, concentrated at the top of the income distribution in a country where the top of the income distribution sits significantly higher than it does anywhere else.
The researchers who published this study were not advocates for physicians. They were economists, doing math. And the math says: cut physician pay dramatically, and you’ve made a dent. A meaningful dent, but a dent. The structural drivers of US healthcare cost are elsewhere — in administrative complexity, in drug pricing, in fragmentation, in a system that was never designed as a system at all.
Your surgeons know this, somewhere. Most of them just haven’t seen anyone lay it out clearly.
Now you can.
Share This With Your Surgeons
Share this article on LinkedIn. Forward this article to your top accounts. Drop it in a text. Leave it in an email with a two-sentence note: “Thought you’d find this interesting — someone finally did the math.” You don’t need to editorialize. The data speaks for itself.
Your surgeon will notice that you’re paying attention to their world beyond the products you carry. That you understand the pressures they’re under. That you’re someone worth talking to about more than implant specs and pricing.
Those are the relationships that last.
Sources: Buehler, Gottlieb, Hicks, Laun, Palme, Polyakova, Udalova, and Ventura. “International Comparison of Physician Incomes.” NBER Working Paper No. 34956, March 2026.